The usefulness of masks in the prevention of respiratory diseases is something very intuitive. If we want to prevent any agent from infecting us, putting something in front of our mouth and nose can only help. But many intuitive things are not confirmed. That’s why we resort to science and its method to abstract ourselves from our intuitions and beliefs and accept their results.
Thus, besides the fact that there is evidence that its use in a hospital environment and in some other circumstances (caregivers of infected people, people with symptoms) is important, the truth is that, until recently, the use of masks in the community by healthy people was not recommended. Most health care organizations advice, and studies that emerged over many years seemed to give strength to this orientation.
After many decades of facing thousands of epidemics and a few pandemics, in the middle of one, the directions change radically. They are now not only recommended, but in many cases mandatory and seen as a decisive tool in combating the disease.
How was this possible? Was the evidence from the past so fragile? Could we have discovered in a few months what we had missed for so long? Does this virus behave differently than all the others we know? Are there other factors behind these changes?
In this article we will focus, in particular, on the evidence that existed before, and on some others that have emerged in the meantime.
Background
During the first phase of the pandemic in the Northern Hemisphere, official recommendations argued that masks should not be worn by healthy people in the community. They had been advised against for many years. They were only advised to infected people (preferably while travelling home or to health care institutions), or to caregivers who had sick people in their care.
In its document on measures to combat influenza – Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza–, the WHO summarised the evidence that included 10 RCTs (randomised controlled trials), the highest quality scientific studies:
“No evidence has been found that the masks are effective in reducing the transmission of confirmed influenza in the laboratory.
ECDC has a similar position:
Evidence of effectiveness: No tests. The use of masks in public is common in some societies in Asia. It has not been observed that infection rates are lower there. There are some authorities who argue that there may be perverse effects because people may reuse contaminated masks and constant adjustment of masks may result in further contamination of the hands with viruses (p. 9).
O CDC presented similar guidelines to the ECDC and the WHO:
It also referred to the recent systematic review cited and funded by the World Health Organisation (May 2020):
Jingyi Xiao et al. Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings—Personal Protective and Environmental Measures. Policy Review. Volume 26, Number 5—May 2020.
In this review, 10 RCTs reported estimates of the efficacy of face masks in reducing influenza virus infections, confirmed in the laboratory, in the community – literature published between 1946 and 27 July 2018.
“There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.”
“Proper use of face masks is essential because improper use might increase the risk for transmission.”
While mechanistic studies support the potential effect of hand hygiene or facial masks, evidence from 14 randomised clinical trials of these measures does not support a substantial effect on transmission of laboratory confirmed influenza.
Other studies on masks
These studies have been adapted and added to the review by the American Association of Doctors and Surgeons.
Many other systematic reviews and RCT studies had been conducted on masks. Here are some of the more recent ones.
- Radonovich, L.J. et al. (2019) “N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial,” JAMA. 2019; 322(9): 824–833.
As worn by health care personnel in this trial, use of N95 respirators, compared with medical masks, in the outpatient setting resulted in no significant difference in the rates of laboratory-confirmed influenza.
Offeddu, V. et al. (2017) “Effectiveness of Masks and Respirators Against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis,” Clinical Infectious Diseases, Volume 65, Issue 11, 1 December 2017, Pages 1934–1942,
Compared to masks, N95 respirators provided superior protection against clinical respiratory diseases and laboratory confirmed bacteria, but not against viral infections or vital influenza (ILI) diseases. The self-reported evaluation of clinical results was subject to bias.
The evidence of the protective effect of masks or respirators against respiratory infection found was not statistically significant (compared to not wearing a mask)
Smith, J.D. et al. (2016) “Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis,” CMAJ Mar 2016
In the meta-analysis of the clinical studies, we found no significant difference between N95 respirators and surgical masks in associated risk of (a) laboratory-confirmed respiratory infection, (b) influenza-like illness, or (c) reported workplace absenteeism
C Raina MacIntyre et al. (2015) A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ.
It was the only RCT with cloth masks performed (on health professionals).
Cloth masks resulted in significantly higher infection rates than medical masks and also performed worse than the control marker, some of which may have worn masks.
The virus can survive on the surface of facial masks. Self-contamination through repeated use and incorrect exchange is possible. A contaminated cloth mask can transfer pathogens from the mask to the user’s unprotected hands.
Moisture retention, re-use of cloth masks and inadequate filtration can result in an increased risk of infection.
Cloth masks should not be recommended for healthcare professionals, especially in high risk situations.
- bin-Reza et al. (2012) “The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence,” Influenza and Other Respiratory Viruses 6(4), 257–267.
“In 17 eligible studies.none established a conclusive relationship between the use of a mask/breather and protection against influenza infection.“
- Jefferson T, et al. (2011) Physical interventions to interrupt or reduce the spread of respiratory viruses (Review). Cochrane Library.
We included 67 studies including randomised controlled trials and observational studies with a mixed risk of bias.”
“Implementing barriers to transmission, such as isolation, and hygienic measures (wearing masks, gloves and gowns) can be effective in containing respiratory virus epidemics or in hospital wards.”
- Cowling, B. et al. (2010) “Face masks to prevent transmission of influenza virus: A systematic review,” Epidemiology and Infection, 138(4), 449-456. DOI:
None of the reviewed studies showed any benefit in wearing a mask, either to health professionals or to community members in households.
6 studies on the use of face masks, both surgical and N-95 respirators in healthcare professionals and community settings.
The effectiveness of facial masks is likely to be affected by compliance problems in the health environment and the community. Several studies show a lower level of compliance with facial masks or find less acceptability in facial masks compared to hand hygiene behaviours and other non-pharmaceutical interventions.
Jacobs, J. L. et al. (2009) “Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: A randomized controlled trial,” American Journal of Infection Control, Volume 37, Issue 5, 417 – 419.
The use of a face mask by healthcare professionals has not been shown to offer benefits in terms of cold symptoms and confirmed cold.
The standpoint of those responsible for public health
Experts from all over the world were peremptory in not recommending the use of masks in the community.
For example, Fauci, director of the National Institute of Allergy and Infectious Diseases (NIAID) and one of the key members of the White House Coronavirus Task Force, said (in March) in this interview:
“When you’re in the middle of an outbreak, wearing a mask may make people feel a little better and may even block a droplet but it’s not providing the protection people think it’s giving. And often there are unwanted consequences. People keep playing with the mask and keep touching the face”.
Dr. Filipe Froes Pneumologist and consultant to DGS (Portugal Health Organization) said (before the epidemic hit us):
“… I have seen several people in masks on the street, I mean, I work in a hospital, I don’t wear a mask for anything. I wear a mask for the procedures I have to do with my patients…”
Changes of opinion on the use of masks in the community
In early April, the CDC reversed its orientation especially based on the role that symptom-free people can play in the transmission of the disease.
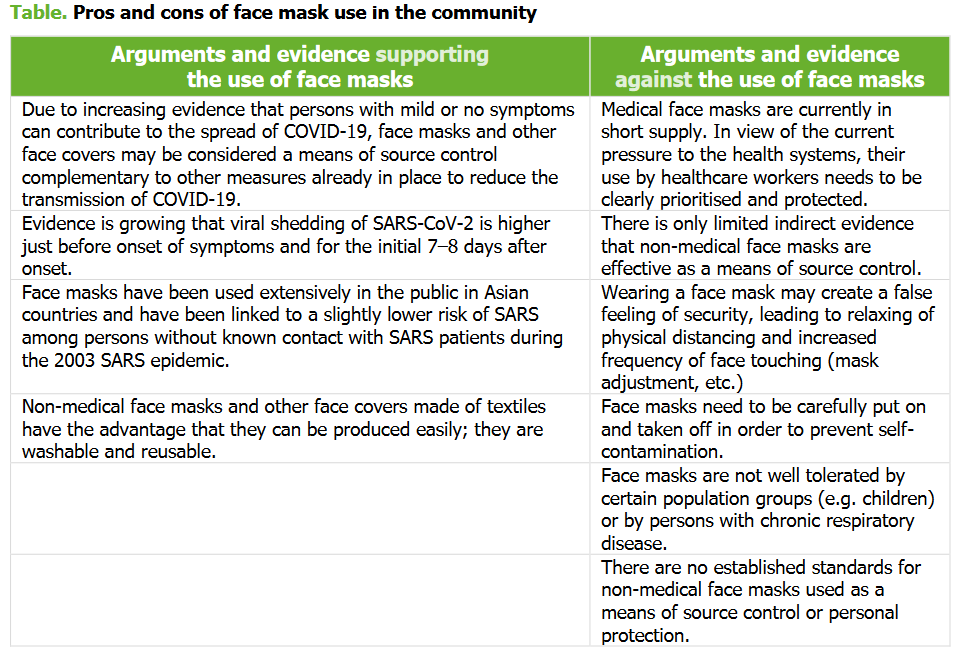
The ECDC also changed its position in April.
The precautions are reflected in this table of advantages and disadvantages of using a community mask (page 3).
In June, the WHO also changed its guidelines. The global health agency now recommends to the public the use of tissue masks (three or more layers) in places where there is widespread transmission of the virus and where physical distance is difficult.
This, while recognizing that there is no evidence to support such measures, either asymptomatic or symptomatic, and basing them on the possibility that the transmission mechanism is the anticipated (mechanistic plausibility).
“While there is no evidence that this is effective in reducing transmission, there is a mechanistic plausibility for the potential effectiveness of this measure”.

Dr. Fauci, for example, in this interview justified the change of position as something normal in science, and justified this position on three points. First of them, one of the reasons for demonstrating against the use of masks was the possibility that this equipment might run out for health professionals. Now there are enough of them. The second point is the idea that cloth masks or household masks “were adequate”. Finally, the fact that 20 to 25% of infected people do not develop symptoms, but they can transmit the disease.
Studies referred to support changes in orientation
The most quoted study by CDCs, WHO, politicians and public health officials was the one that was published in the Lancet:
Chu, D.K. et al (2020). Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet.
For example, the ECDC quotes it first in the list of evidence for the measure:
Evidence basis for the measure
There is increasing evidence showing the effect of facial masks on the prevention of transmission of SARS-CoV-2. In a recent systematic review, Chu et al. determined that, on average, there was more than five-fold reduction in the risk of transmission, from 17.4% without a face mask to 3.1% with a 1216-layer cotton mask (e.g. N95, surgical or cotton mask).
Despite its popularity, and having supported many of the changes made in terms of international recommendations, it has been greeted with scepticism by many professionals in the scientific community.
A summary of some of the criticisms:
- The majority of studies (two thirds) are on MERS and SARS-CoV-1. This should be mentioned in the title instead of just SARS-CoV-2 and Covid-19. The WHO itself describes the study as “a systematic review of observational studies related to betacoronaviruses”.
- There seems to be a bias in the selection of studies. In more than 20,000 studies they found, they focused on 172 and 44 studies for meta-analysis. This selection did not result in studies with a high degree of evidence, only in studies with a lower level of evidence.
- None of the studies included is RTC (randomized and controlled study) – the level of evidence with minor biases, and the only one that allows determining causality relationships.
- The selected observational studies are retrospective and based heavily on reports and memories, which makes them even less reliable. In one of the studies, the author states: “However, we found it difficult in our study to obtain a precise exposure history of individuals, some of whom attended more than one patient and all of whom had an imperfect connection at an extremely stressful time”.
- Most of them have not been peer reviewed or published.
- Of the 44 meta-analysis studies only seven were with Sars Cov-2. Of these, only 3 had been published and 4 had been neither peer-reviewed nor published.
- The overall quality of studies is considered quite low and has numerous serious shortcomings, even in relation to other interventions that it intends to measure
- There is insufficient evidence to support the claim that surgical masks can greatly reduce infections (unlike N-95, where there appears to be some evidence)
- Although the study is used to guide global face mask policy for the general population, only three of the 29 meta-analysis studies were conducted in the community. None of these studies refers to SARS-CoV-2.
- Virtually all studies concern indoor spaces with many hours of exposure and in a hospital setting, a distinct context from community use, especially outdoors.
- Almost all the participants in the 29 studies were health workers, trained to wear masks correctly and provided daily with clean masks. This was quite distinct from community use by untrained staff.
The WHO, in its “Advice on the use of masks in the context of OVID-19- Interim guidance” (5 June 2020), also invokes it to highlight its findings, but stressed the weak level of evidence presented.
Evidence of low certainty – from a systematic review of observational studies related to betacoronaviruses that cause severe acute respiratory syndrome (SARS), Middle Eastern respiratory syndrome (MERS) and COVID-19 – has shown that the use of face protection (including respirators and medical masks) results in a greatly reduced risk of infection among health care professionals. N95 or similar respirators may be associated with a greater reduction in risk when compared to 12-16 layer medical or cotton masks). But the studies had important limitations (memory bias, limited information on the situations in which respirators were used and on the measurement of exposures), and many of them were carried out in environments where GPA (procedures that provide greater generation of aerosols) were performed. (page 3)
The authors themselves, in their summary table, acknowledge that the degree of reliability for the suggested conclusions is low.

Other studies cited to justify the change of position
One of the most used studies was that of Missouri hairdressers who were infected with SARS-CoV-2. They wore masks and their customers were not infected. (July 2020)
The conclusion drawn by the CDC was that “Adherence to the community’s and company’s face-covering policy likely mitigated spread of SARS-CoV-2.”.
There are other clear limitations: this is a case study (low level of evidence), and other measures were in place to prevent prolonged close contact. In other words, the fact that the subjects did not transmit the virus does not allow us to extrapolate that it was due to the mask.
There are many cases of infected people who do not cause disease (or infection) in their close contacts, even if they are in prolonged contact with them.
In this study, one asymptomatic person, infected with Covid, did not infect 455 people with whom he was in contact.
Thus, if the mask had been the reason that the two symptomatic subjects didn´t infected a third party, this could reinforce the previous orientation for its use in case of illness. Given that there are numerous cases of asymptomatic non transmitters, it cannot be presented as evidence that asymptomatics should also use it.
Other studies cited are of a low or medium level of evidence. Some present some serious problems.
For a brief analysis of some of these studies see, for example, the review by the American Association of Physicians and Surgeons.
General considerations
The change in direction may have had positive aspects:
- It certainly helped many people to have the confidence to leave home and return to some normality in their lives
- There are still some uncertainties, for example as to the relevance of pre-symptomatics persons. It may therefore make sense in some circumstances (closed spaces, lack of ventilation, long contacts) to recommend it, along with other measures
However, there are also some negative points:
- Little concern and investment in raising awareness of the correct use of masks, knowing that there are numerous risks associated with their misuse, is a worrying sign and may indicate that they are be being used for other purposes.
- For example, cloth masks which, from (little) existing research, appear to be able to contribute to a higher rate of user infection, have laboratory evidence that they may only have a multi-layered effect (minimum 3) and specific characteristics. However, this has also not been passed on to the population who continue to wear, in many cases, simple cloth masks without any particular care.
Whatever considerations we may make, the reality is that after many decades of opposing the use of masks in the community (by healthy people), the world’s major health entities have changed their viewpoints. The WHO more cautiously, the CDC and the ECDC more categorically.
Many countries have changed their policies. Some have made it mandatory in some circumstances in indoors or even outdoors. Others, like the Nordics, have changed little or nothing in their policies on masks.
As the WHO recognises, there remains little evidence to support the widespread use of masks in communities (especially outdoors). The previous evidence appears to be much more robust and of higher quality.
However, it is also not perfect and is susceptible to change. In this infection there are also possible particularities, such as greater transmission by pre-symptoms, which may justify specific guidelines.
More and better studies are certainly needed. Here, as in other areas, it is essential not to have closed positions so that new evidence can be incorporated. Only in this way can we take advantage of the great advance that the scientific method represents and avoid falling into obscurantism.
Different expert opinions on masks
Carl Heneghan
British General Practitioner, Director of the Centre for Evidence Based Medicine at Oxford University and member of Kellogg College. Editor-in-Chief of BMJ Evidence-Based Medicine
Larry Chu
Doctor in charge of the Anesthesia Informatics and Media (AIM) laboratory at Stanford University. Professor of Anesthesiology, Perioperative and Pain Medicine. Executive Director of Stanford Medicine.
Jay Bhattacharya
Senior associate at the Freeman Spogli Institute for International Studies. Professor of Medicine. Senior fellow at Stanford Institute for Economic Policy Research. Director of the Medical Outcomes Programme. Director of the Centre for Demography and Economics of Health and Ageing. Member of the faculty of the Center for Health Policy and the Center for Primary Care and Outcomes Research.
Lisa Maragakis
Senior infection prevention director, The Johns Hopkins Health System. Associate Professor of Medicine










